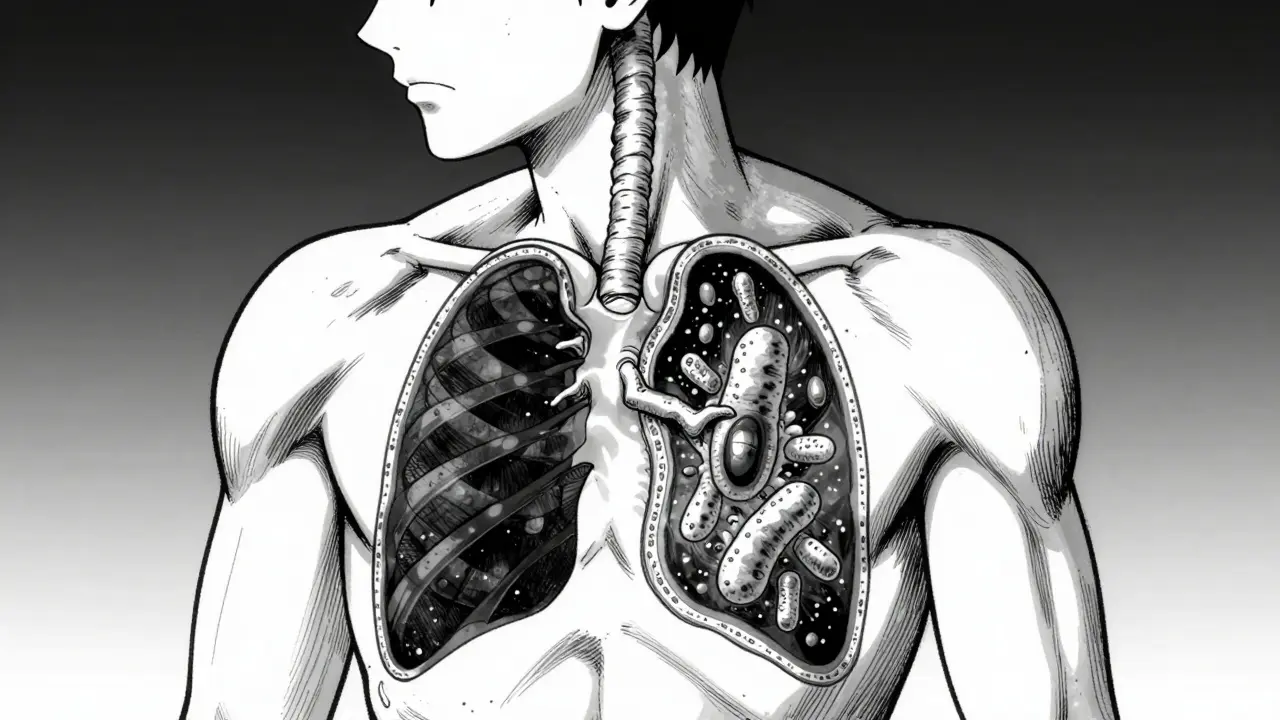
Imagine carrying a seed in your body that stays dormant for decades, never causing a single sneeze or cough, only to bloom into a serious illness years later when your defenses drop. That is exactly how Tuberculosis is a severe infectious disease caused by the bacterium Mycobacterium tuberculosis that primarily attacks the lungs. While many people think of TB as a relic of the 19th century, it remains a top ten cause of death globally. The real danger lies in the fact that you can be infected without ever feeling sick, creating a massive hidden reservoir of bacteria waiting for the right moment to strike.
The Invisible Phase: Latent TB Infection
When Mycobacterium tuberculosis enters the body, it doesn't always cause immediate chaos. In many cases, the immune system manages to wall off the bacteria, creating a state of equilibrium. This is known as Latent TB Infection (LTBI). In this state, the bacteria are alive but inactive. You aren't coughing, you don't have a fever, and most importantly, you cannot spread the bacteria to anyone else.
For most people, this is a lifelong stalemate. About 30% of people exposed to TB will show signs of infection on a test, but only a small fraction will ever get sick. However, the "latent" label can be deceiving. It isn't a permanent cure; it's a truce. If your immune system weakens-perhaps due to aging, chronic illness, or an untreated HIV infection-the bacteria can break through those walls and start multiplying. About 10% of people with latent TB will develop active disease at some point in their lives, though that number jumps significantly for those who are immunocompromised.
When the Balance Shifts: Active TB Disease
Active TB is what most people picture when they hear about the disease. This occurs when the bacteria overcome the body's defenses and begin destroying tissue. Unlike the latent phase, Active TB Disease is characterized by reproducing bacteria that cause systemic illness and are highly contagious.
The symptoms don't usually hit you like a ton of bricks; they creep up over several weeks. You might start with a persistent cough that lasts more than three weeks. As the infection progresses, you'll likely notice unexplained weight loss and drenching night sweats-sometimes so severe that you have to change your clothes or sheets in the middle of the night. Fever, chills, and fatigue follow. In advanced pulmonary cases, you might experience hemoptysis, which is the medical term for coughing up blood, along with sharp chest pain.
How Doctors Tell the Difference
Diagnosing TB isn't as simple as a single test because the approach depends entirely on whether the infection is latent or active. To identify latent TB, doctors rely on immunologic tests like the Tuberculin Skin Test (TST) or the Interferon-Gamma Release Assay (IGRA). If these are positive, but your chest X-ray is clear and you have no symptoms, you have LTBI.
Active TB requires a much more aggressive diagnostic path. A positive skin test isn't enough; doctors need microbiological confirmation. This usually involves a sputum culture-testing the mucus you cough up-to see if the bacteria actually grow in a lab. Modern clinics also use nucleic acid amplification tests (NAAT), which can detect the bacterial DNA quickly, allowing for faster treatment starts.
| Feature | Latent TB Infection (LTBI) | Active TB Disease |
|---|---|---|
| Contagious? | No | Yes (Pulmonary) |
| Symptoms | None | Cough, fever, weight loss, night sweats |
| Chest X-ray | Typically normal | Typically abnormal |
| Tests | Positive TST/IGRA | Sputum culture or NAAT positive |
| Treatment Goal | Prevent progression to active | Cure disease and stop transmission |
Tackling the Bacteria: Drug Therapy
Treating TB is a marathon, not a sprint. Because the bacteria are stubborn and can hide in different parts of the body, the drug regimens are long and intensive. The biggest risk in TB therapy is drug resistance; if a patient stops taking their meds too early, the surviving bacteria evolve into multidrug-resistant TB (MDR-TB), which is far harder to treat.
For those with latent TB, the goal is to kill the dormant bacteria before they wake up. This is usually done with a single medication, often Isoniazid, for about nine months. However, newer, shorter regimens are becoming more common to help people finish their treatment. For example, some patients may use a combination of isoniazid and rifapentine for just three months.
Active TB requires a heavy-hitting approach. The standard strategy uses a four-drug cocktail: Isoniazid, Rifampin, Pyrazinamide, and Ethambutol. This combination is used for the first two months to knock down the bacterial load quickly. After that, the patient moves to a continuation phase using just isoniazid and rifampin for another four to seven months.
Because these drugs can be hard on the liver (hepatotoxicity), doctors perform regular liver function tests throughout the process. To ensure no one misses a dose, health departments often use Directly Observed Therapy (DOT), where a healthcare worker actually watches the patient swallow their medication.

The Complex Biology of TB Control
The struggle between the human body and TB is a fascinating biological battle. When you have latent TB, your body creates what is called a granuloma-a specialized clump of immune cells that essentially cages the bacteria. This keeps the infection in a state of equilibrium. Research shows that in latent cases, the body utilizes specific CD8 T cells that are highly specialized in maintaining this containment.
When that equilibrium breaks, it's often because the immune system can no longer maintain the granuloma. This allows the bacteria to spill out and multiply rapidly. Interestingly, some researchers argue that TB isn't just a "yes or no" switch between latent and active. They suggest there is a spectrum of infection, where some people exist in a "smoldering" state that is more than latent but not yet fully active disease.
Can I spread TB if I have a latent infection?
No. If you have latent TB, the bacteria are inactive and contained within your body. You cannot cough them into the air, meaning you pose no risk of transmission to friends, family, or coworkers.
Why do I need treatment if I feel perfectly fine with latent TB?
Treatment for latent TB is preventative. Since you are already infected, there is a lifelong risk that the bacteria could become active. Taking medication now prevents you from becoming seriously ill in the future and prevents you from becoming contagious.
Is tuberculosis curable?
Yes, TB is curable with the correct course of antibiotics. The key is strict adherence; skipping doses can lead to the development of drug-resistant strains, which are much more difficult and expensive to treat.
How is active TB transmitted?
Active pulmonary TB is spread through respiratory droplets. When an infected person coughs, sneezes, sings, or talks, they release tiny droplets containing Mycobacterium tuberculosis into the air, which can then be inhaled by people nearby.
What are the most common side effects of TB drugs?
The most significant concern is liver toxicity, which is why doctors monitor liver enzymes. Some patients may also experience joint pain, nausea, or changes in vision (specifically with ethambutol), making regular medical check-ups essential.
Next Steps for Management
If you have been exposed to someone with active TB, the first step is to get an IGRA blood test or a skin test. If the result is positive, don't panic-you are likely in the latent phase. Schedule a chest X-ray to confirm there is no active disease. Depending on your health status, your doctor will decide if preventative therapy (like isoniazid) is necessary.
For those already undergoing active TB treatment, the most critical step is to never stop your medication without a doctor's order, even if you start feeling better after a few weeks. If you notice yellowing of the eyes (jaundice) or dark urine, contact your provider immediately, as these are signs of liver stress.



